In the dynamic environment of a healthcare practice, precise and thorough documentation is not merely a formality; it is the cornerstone of effective patient care, legal protection, and efficient operations. Every patient encounter, from a routine check-up to a complex diagnostic consultation, generates a wealth of critical information that must be meticulously recorded. A robust Medical Office Note Template serves as the fundamental tool for achieving this, providing a structured framework that guides practitioners in capturing essential details consistently and comprehensively.
The process of creating and maintaining accurate medical records can be time-consuming and prone to inconsistencies if left to individual discretion. Without a standardized approach, vital information might be overlooked, leading to potential misdiagnoses, suboptimal treatment plans, or administrative errors. Templates address these challenges head-on by streamlining the documentation process, ensuring that all necessary data points are considered and recorded in a uniform manner, regardless of the practitioner or the specific patient visit.

Beyond the immediate clinical benefits, well-structured medical notes are indispensable for a multitude of reasons. They facilitate clear communication among healthcare providers involved in a patient's care, serve as crucial evidence in medico-legal contexts, support billing and coding accuracy, and provide valuable data for quality improvement initiatives and research. The quality of these notes directly impacts the quality of care delivered and the operational efficiency of the entire medical office.
This article delves into the critical role of a medical office note template, exploring its components, benefits, and best practices for its implementation. We will examine how a thoughtfully designed template can transform daily documentation tasks, enhance clinical accuracy, improve patient outcomes, and contribute to a more organized and compliant healthcare practice. Understanding the nuances of these templates is essential for any medical professional looking to optimize their record-keeping.

The Indispensable Role of Medical Documentation
Medical documentation is far more than just writing down observations; it is the official, legal record of a patient's medical history, clinical findings, diagnostic tests, treatment plans, and responses to care. It serves as a continuous narrative of a patient's health journey within a specific practice or healthcare system. Every entry must be accurate, legible, timely, and complete, reflecting a clear picture of the patient's condition and the care provided.
Effective documentation supports continuity of care, allowing different healthcare professionals to understand the patient's history and current status without needing to repeat investigations or gather information afresh. It also plays a crucial role in patient safety, as accurate records help prevent medication errors, allergic reactions, and ensure appropriate follow-up. In the event of a medical audit or legal challenge, comprehensive notes are the primary source of defense, demonstrating adherence to professional standards and due diligence.

Furthermore, medical notes are vital for administrative and financial aspects of healthcare. They provide the necessary information for accurate medical coding and billing, ensuring that services rendered are correctly charged and reimbursed. They also contribute to data collection for public health monitoring, research studies, and quality assurance programs, driving advancements in medical science and improvements in healthcare delivery.
Why Standardized Documentation Matters
Standardization in medical documentation is key to overcoming challenges associated with varying individual styles and levels of detail. Without a consistent framework, notes can become difficult to read, interpret, and compare across different visits or providers. This lack of uniformity can lead to miscommunication, errors, and inefficiencies, ultimately impacting patient care and practice productivity.

A standardized approach, often facilitated by a robust Medical Office Note Template, ensures that all critical information is consistently captured in a logical and accessible format. It minimizes the risk of omission, promotes clarity, and streamlines the review process. This consistency is particularly important in multi-provider practices or when patients receive care from different specialists, as it fosters seamless information exchange and collaborative decision-making.

Key Components of an Effective Medical Office Note Template
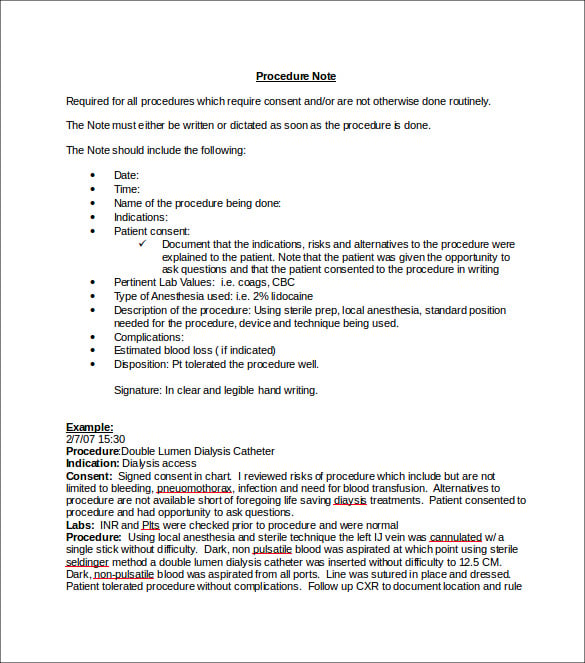
An effective Medical Office Note Template is designed to capture all relevant clinical and administrative information required for a complete patient record. While the specific layout and content may vary based on specialty and practice preferences, several core components are almost universally included.

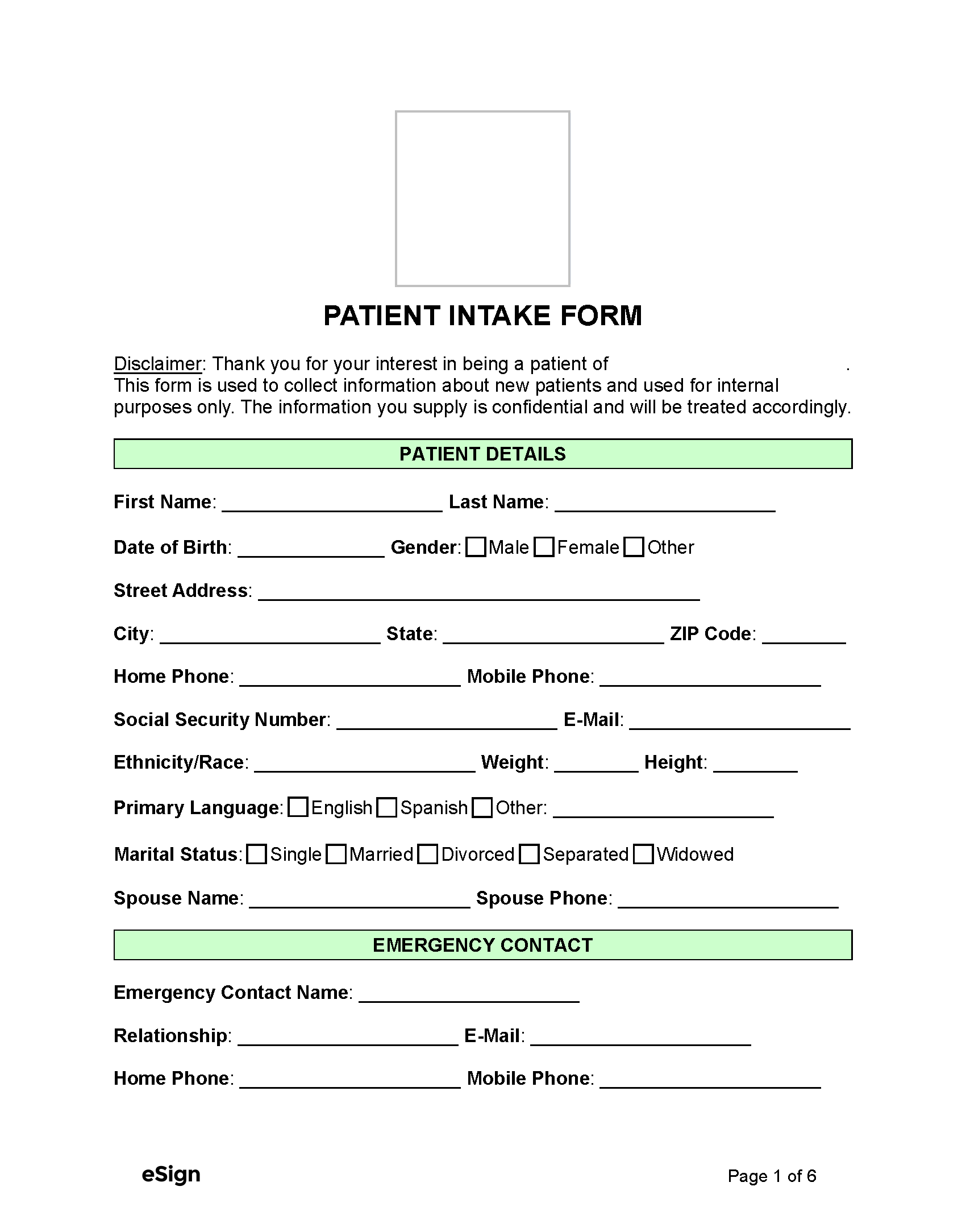
Patient Demographics and Administrative Information
Every note begins with identifying information to ensure the record belongs to the correct patient. This typically includes:
* Patient Name, Date of Birth, and Medical Record Number (MRN): Essential for accurate identification.
* Date and Time of Visit: Crucial for chronological tracking.
* Provider Name and Signature/Electronic Signature: Identifies the author of the note.
* Chief Complaint (CC): The primary reason for the patient's visit, often stated in their own words.

Subjective (S) Data
The "Subjective" section, often associated with the SOAP note format, captures information reported directly by the patient or their family. This is the patient's story in their own words, detailing their symptoms, feelings, and relevant history.
* History of Present Illness (HPI): A detailed account of the chief complaint, including its onset, duration, location, character, aggravating/alleviating factors, radiation, and temporal sequence (OLD CARTS).
* Review of Systems (ROS): A comprehensive inquiry about the patient's current health status across various body systems (e.g., cardiovascular, respiratory, gastrointestinal).
* Past Medical History (PMH): Significant past illnesses, hospitalizations, surgeries.
* Family History (FH): Relevant medical conditions in close relatives.
* Social History (SH): Lifestyle factors such as occupation, living situation, smoking, alcohol use, drug use, diet, exercise.
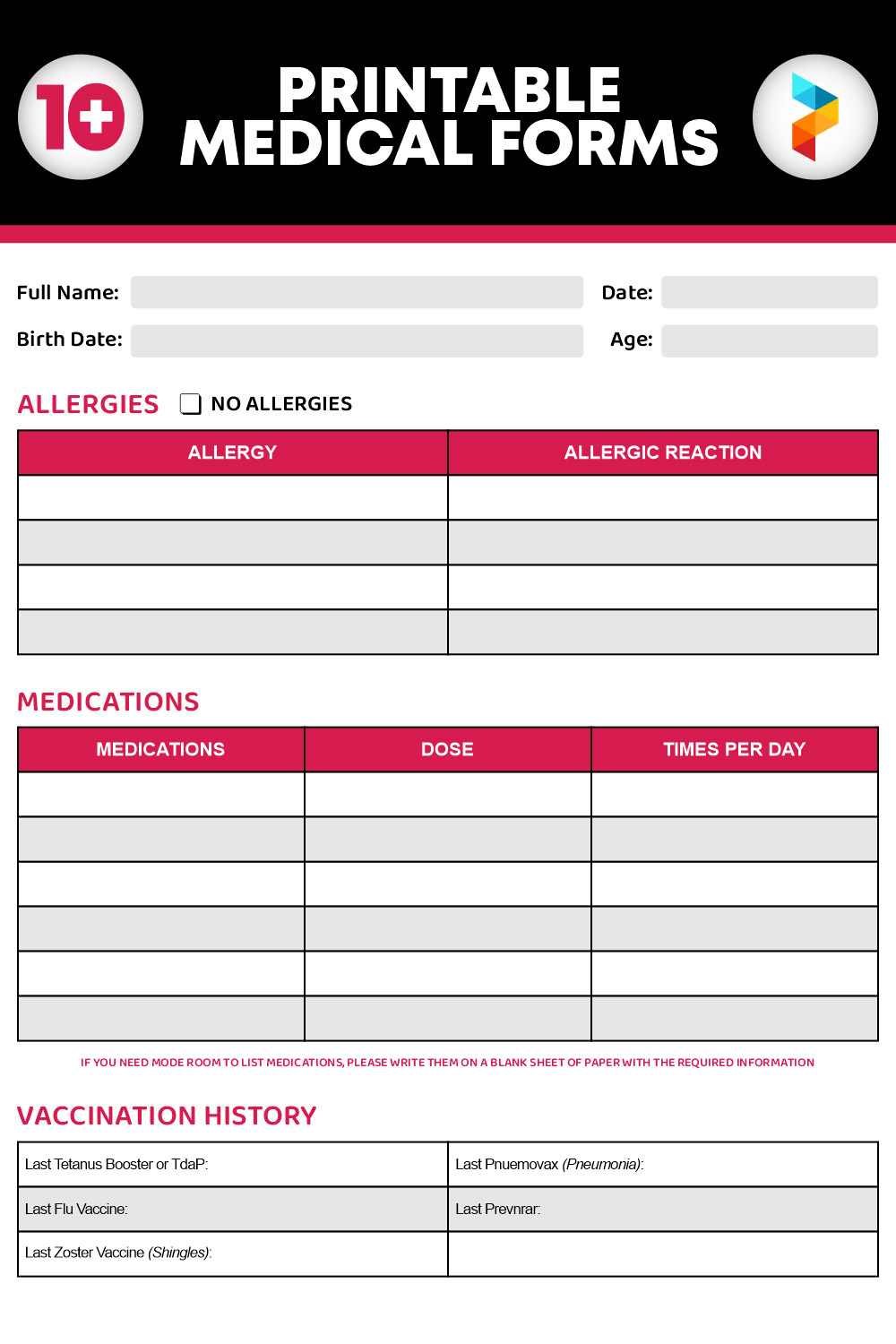
* Medications and Allergies: Current medications (including over-the-counter and supplements) and known allergies with reactions.
Objective (O) Data
The "Objective" section contains factual, measurable, and observable information gathered by the healthcare provider during the examination.
* Vital Signs: Temperature, blood pressure, heart rate, respiratory rate, oxygen saturation, weight, height.
* Physical Examination (PE): Findings from a systematic head-to-toe examination, focusing on areas relevant to the chief complaint and ROS.
* Diagnostic Test Results: Lab results, imaging reports (X-rays, MRI, CT scans), EKG findings, and other objective data that support or rule out diagnoses.
Assessment (A)
The "Assessment" section is the provider's professional interpretation of the subjective and objective data.
* Problem List/Diagnosis: A summary of the patient's active medical problems and their corresponding diagnoses (e.g., ICD-10 codes). These may be ranked by severity or priority.
* Differential Diagnoses: Other possible conditions considered but ruled out.
Plan (P)
The "Plan" section outlines the course of action based on the assessment.
* Therapeutic Interventions: Medications prescribed, treatments initiated, referrals made.
* Diagnostic Studies: Further tests ordered (labs, imaging, consultations).
* Patient Education and Counseling: Information provided to the patient regarding their condition, medications, lifestyle modifications, and self-care.
* Follow-up Instructions: When and why the patient should return, or under what circumstances they should seek immediate care.
Customizing Your Medical Office Note Template for Specialty Practice
While the core components of a medical note remain consistent, the most effective Medical Office Note Template is often tailored to the specific needs of a medical specialty. A primary care template, for example, will differ significantly from one used in cardiology, dermatology, or orthopedics.

For a cardiologist, the template might emphasize detailed cardiovascular history, EKG findings, echocardiogram reports, and specific parameters like ejection fraction. A dermatologist's template would focus on skin lesions, their morphology, distribution, and dermatoscopic findings. Orthopedists would require specific sections for musculoskeletal examination, range of motion, and imaging of bones and joints.

Customization allows practitioners to:
* Streamline relevant data capture: Eliminating unnecessary fields and emphasizing critical ones.
* Improve efficiency: Reducing time spent on documentation by providing pre-populated fields or dropdown menus for common findings and treatments in that specialty.
* Enhance accuracy: Ensuring that specialty-specific diagnostic criteria and treatment protocols are consistently addressed.
* Support compliance: Incorporating regulatory requirements specific to the specialty, such as detailed reporting for certain procedures or conditions.

When customizing a template, it is important to involve all relevant staff, including physicians, nurses, and medical assistants, to ensure it meets the practical needs of the entire team. Regular review and updates are also crucial to adapt to evolving clinical guidelines, technological advancements, and regulatory changes.

Implementing Digital Medical Office Note Templates
The transition from paper-based to digital documentation, primarily through Electronic Health Records (EHR) or Electronic Medical Records (EMR) systems, has revolutionized the use of Medical Office Note Templates. Digital templates offer significant advantages over their paper counterparts.
Advantages of Digital Templates:
- Accessibility: Notes can be accessed instantly from any authorized location, facilitating remote care and inter-departmental collaboration.
- Legibility: Eliminates issues with handwriting, ensuring all entries are clear and readable.
- Searchability: Allows for quick retrieval of specific information within a patient's record or across a patient population for research or audits.
- Integration: Can be integrated with other parts of the EHR/EMR, such as lab results, imaging, and billing systems, creating a holistic patient record.
- Automation: Pre-populated fields, dropdown menus, and smart-text features (macros) speed up documentation.
- Error Reduction: Built-in alerts and prompts can reduce the likelihood of critical omissions or errors.
- Security: Digital records offer enhanced security features (encryption, access controls) compared to physical charts, aiding HIPAA compliance.
- Data Analytics: Facilitates the extraction of data for quality improvement, research, and population health management.
Challenges and Considerations for Digital Implementation:
- Initial Setup and Customization: Requires significant upfront effort to configure templates to meet practice-specific needs.
- Training: Staff training is essential to ensure proficient use of the EHR/EMR system and its templates.
- Interoperability: Ensuring seamless data exchange between different systems can still be a challenge.
- "Click Fatigue": Over-reliance on structured templates can sometimes lead to excessive clicking and data entry, potentially impacting the narrative quality of notes. Striking a balance between structured data and free text is crucial.
- Cost: Implementing and maintaining an EHR/EMR system with robust template capabilities can be a significant financial investment.
Legal and Compliance Aspects of Medical Notes
Medical office notes are legal documents that can be subpoenaed in court, making their accuracy and completeness paramount. Adherence to strict legal and ethical guidelines is non-negotiable.
HIPAA and Patient Privacy
The Health Insurance Portability and Accountability Act (HIPAA) mandates strict rules regarding the privacy and security of patient health information (PHI). All medical notes, whether paper or digital, must be protected from unauthorized access or disclosure. Templates should be designed to support HIPAA compliance by facilitating secure documentation practices and ensuring that only authorized personnel can view or modify records.
Documentation Standards
Healthcare providers are held to professional standards of documentation. Notes must be:
* Accurate: Reflecting the true clinical picture.
* Complete: Containing all relevant information about the patient encounter.
* Legible: Easily readable (especially important for paper notes).
* Timely: Recorded promptly after the encounter.
* Attributable: Clearly indicating who made the entry.
* Authentic: Verified by signature or electronic authentication.
Incomplete or poorly documented notes can lead to legal liabilities, payment denials from insurers, and compromise patient safety. A well-designed Medical Office Note Template acts as a guardian, reminding practitioners of essential fields and prompting complete data capture, thereby bolstering compliance and legal defensibility.
Best Practices for Using and Optimizing a Medical Office Note Template
Maximizing the utility of a medical office note template requires more than just its creation; it demands thoughtful implementation, ongoing training, and continuous refinement.
Training and Standardization Across Staff
Effective template use relies on consistent application by all staff members. Regular training sessions should be conducted to ensure everyone understands how to use the template correctly, including specific fields, required elements, and any specialty-specific nuances. Standardizing the interpretation and input of information minimizes variability and enhances data quality.
Regular Review and Updates
Medical knowledge, clinical guidelines, and regulatory requirements are constantly evolving. A static template quickly becomes outdated. Schedule periodic reviews (e.g., annually or semi-annually) to:
* Incorporate new best practices: Add fields for emerging treatments or diagnostic criteria.
* Remove obsolete sections: Eliminate information that is no longer relevant.
* Address user feedback: Modify the template based on suggestions from practitioners to improve usability and efficiency.
* Ensure compliance: Update in response to changes in billing codes (ICD, CPT), HIPAA regulations, or other legal requirements.
Balancing Structure with Narrative Freedom
While templates are designed to provide structure, it's crucial to avoid "template fatigue" where notes become generic and lack individualized patient details. Encourage practitioners to use the structured fields for objective data but also utilize free-text areas to add personalized narrative, nuanced observations, and the patient's unique story. This balance ensures both comprehensive data capture and rich clinical context.
Leveraging Technology Features
Modern EHR/EMR systems offer advanced features that can significantly enhance template use:
* Voice Recognition Software: Converts spoken words into text, speeding up documentation.
* SmartPhrases/Macros: Pre-defined text snippets or paragraphs that can be inserted with a few keystrokes, ideal for common patient education or recurring symptoms.
* Problem-Oriented Templates: Templates that dynamically adapt based on the patient's active problem list.
* Flowsheets: Visual representations of data over time, useful for tracking chronic conditions.
Utilizing these features can drastically reduce documentation time, allowing providers to focus more on patient interaction.
Conclusion
The Medical Office Note Template is an indispensable tool in modern healthcare, serving as the backbone for efficient, accurate, and compliant clinical documentation. From streamlining patient encounters and ensuring continuity of care to safeguarding legal interests and facilitating accurate billing, its impact is far-reaching. By providing a structured framework, these templates help healthcare professionals capture critical subjective and objective data, formulate precise assessments, and develop comprehensive treatment plans.
Whether in a paper-based system or integrated within an advanced Electronic Health Record, a well-designed template enhances the quality of patient records, improves communication among care providers, and supports adherence to legal and regulatory standards like HIPAA. The key to maximizing its benefits lies in thoughtful customization for specialty needs, diligent staff training, and a commitment to ongoing review and optimization. Embracing a robust and intelligently utilized medical office note template is not just about better record-keeping; it's about fostering superior patient care, operational efficiency, and a resilient healthcare practice.
0 Response to "Medical Office Note Template"
Posting Komentar